1. Introduction
The opioid epidemic presents a persistent and growing threat. As of 2023, approximately 10 million U.S. adults misuse opioids annually, resulting in nearly 50,000 deaths per year.1,2 Beyond this staggering mortality rate, opioid use disorder (OUD) carries broader social costs, such as relational and familial damage, reduced employment and economic stability, and increased risk of crime.3,4 Recently, research has begun to identify the links between OUD and other mental health disorders, such as posttraumatic stress disorder (PTSD) and depression, and to investigate the impact of co-morbidity on treatment access and effectiveness.5–7 Given that patients with co-occurring disorders (COD) often experience more severe clinical profiles and report higher rates of suicidal ideation and behavior, access to prompt and effective treatment – including medication for opioid use disorder (MOUD) and counseling or medication for mental health disorders – is essential.8
For individuals in need of such care, research has consistently identified discrepancies between non-Hispanic white patients and ethnically minoritized patients in access to and utilization of treatment for OUD and mental health disorders.9–12 For instance, while Hispanic/Latinx populations have the highest proportion of youth with OUD, they are less likely to access MOUD in their community health care settings, less likely to be referred for OUD treatment or prescribed MOUD, and less likely to complete treatment if initiated.9–12 Similarly, non-Hispanic white individuals are more than twice as likely as Hispanic/Latinx individuals to receive outpatient care for mental health concerns, and among those who receive treatment, non-Hispanic White patients are significantly more likely to receive psychotropic medication.13 Notably, many of these disparities exist among patients who are already enrolled in primary care settings or have at least annual contact with a primary care provider.9–13
Such disparities have been attributed to multiple socioeconomic and systemic factors. Minoritized patients are more likely to hold lower socioeconomic status, which can involve more challenges affording health care and attending regular appointments.14–16 Furthermore, due to provider bias, minoritized patients may be treated differently from White patients, which, over time, erodes trust in health care providers and the treatment plans they propose, and therefore makes minoritized patients more likely to refuse standard services and engage less frequently with mainstream health care providers.17 Institutional medical racism and systemic biases, such as differences in securing health insurance (lower rates among Black and Hispanic/Latinx patients compared to non-Hispanic White patients)18–20 and differences in distribution of resources (i.e., facilities in minoritized communities suffering from lower staffing)19 continue to be problematic across the U.S. and leave patients of color with poorer access to health care. Thus, while not attributable to any one individual, institutional medical racism can have wide-reaching consequences on the practical delivery of health care treatment.18–20
Given the range of such socioeconomic and systemic inequity that minoritized persons contend with, it remains essential to identify and rectify disparities in utilization of health care. To date, little is known about racial and ethnic disparities in utilization of care for individuals with COD specifically. Because prompt and effective treatment is essential to prevent morbidity and mortality in this population, it is vital to highlight any existing disparities and rectify their causes.8 Left unchecked, ethnic disparities in utilization of care for COD mean that minoritized communities will disproportionately bear the burden of untreated COD, resulting in higher rates of social isolation, stigmatization, and financial insecurity, as well as illness and death – all of which may contribute to wider ongoing social inequality.3
The current study examined ethnic patterns in utilization of care for primary care patients in New Mexico with co-occurring OUD and depression and/or PTSD. The primary aim of this study was to identify whether disparities in utilization of mental health and substance-use treatment exist between Hispanic/Latinx and non-Hispanic/Latinx primary care patients with co-occurring disorders in New Mexico.
2. Methods
Procedures
Data for this study were part of a larger randomized pragmatic trial entitled Collaboration Leading to Addiction Treatment and Recovery from Other Stressors (CLARO). CLARO is testing whether the collaborative care model is more effective than usual care for treating patients in New Mexico with co-occurring OUD and depression and/or PTSD.21 Because CLARO captured data relevant to multiple forms of treatment for COD and occurred in a landscape with a high percentage of Hispanic/Latinx individuals, it was deemed an appropriate data source for this research. Patients with probable OUD, depression and/or PTSD were recruited for the trial from 14 low-resourced rural and urban primary care clinics in three health systems in New Mexico between October 2020 and December 2023. Recruitment occurred through a combination of provider referrals, clinic waiting room screening, and self-referrals from recruitment flyers posted in waiting rooms and exam rooms. Recruited patients were screened for eligibility, and if eligible, enrolled and randomized.
Immediately after enrollment in the trial, participants completed a comprehensive baseline interview, which included questions about demographics, mental health symptoms, opioid use, prior treatment for mental health disorders and OUD, and social determinants of health. Baseline interviews were conducted verbally and immediately documented in writing by research assistants in a private clinic room. The study was approved by the RAND Corporation’s institutional review board (IRB no. 2019-0509), and additional details about the study are available in the protocol paper.21
Measures
All variables were self-reported by patients during their baseline interviews. We analyzed two dependent variables: prior utilization of 1) MOUD and 2) mental health treatment. We defined prior utilization of MOUD as consumption of buprenorphine or methadone only as prescribed in the 30 days prior to baseline. We defined prior utilization of mental health treatment as receipt of prescription medications, counseling, or both for depression and/or PTSD in the 30 days prior to baseline. Data were collected pertaining to these dependent variables through specific questions in the baseline interview (see Appendix).
Our primary independent variable was a binary indicator of ethnicity, with values of Hispanic/Latinx or not Hispanic/Latinx. We also included demographics: age, sex, race (white or non-white), education, marital status, and probable diagnosis group (OUD with depression only, OUD with PTSD only, OUD with depression and PTSD). Lastly, we included a variable to indicate the presence of a social support person in participants’ lives, as social support has been found to improve patients’ utilization of health care treatment.22 All of these variables were collected through the baseline interview.
Data Analysis
We used t-tests to compare unadjusted differences in age and chi-square tests to examine unadjusted differences in education, race, sex, marital status, social support, and diagnosis group between Hispanic/Latinx and non-Hispanic/Latinx patients. To reduce the likelihood of falsely identifying significant results due to multiple comparisons (Type I error), we applied the Benjamini-Hochberg correction with a false discovery rate (Q = 0.05).23
Additionally, we used logistic regression to analyze and compare the likelihood of receiving medications for opioid use disorder (MOUD) and mental health treatment between Hispanic/Latinx and non-Hispanic/Latinx patients, adjusting for health system, age, education, sex, race, marital status, and diagnosis group. We report recycled predicted means with 95% confidence intervals (CI) from each of these models to illustrate rates by group after adjustment. Data management was done in SAS 9.4, and statistical tests were conducted in Stata 17.
3. Results
The sample for this study included 736 participants; 516 (70.1%) participants identified as Hispanic/Latinx, and 220 (29.9%) did not. Table 1 compares patient characteristics by ethnicity.
A higher proportion of non-Hispanic/Latinx patients identified as white (76.5%) compared to Hispanic/Latinx patients (59.5%). Hispanic/Latinx patients were more likely (90.5%) than non-Hispanic/Latinx patients (82.3%) to report the presence of a significant social support person in their lives, and Hispanic/Latinx patients were more likely than non-Hispanic/Latinx patients to report a lower level of education completed at the time of the study. There were no other statistically significant differences by ethnicity in the unadjusted analysis.
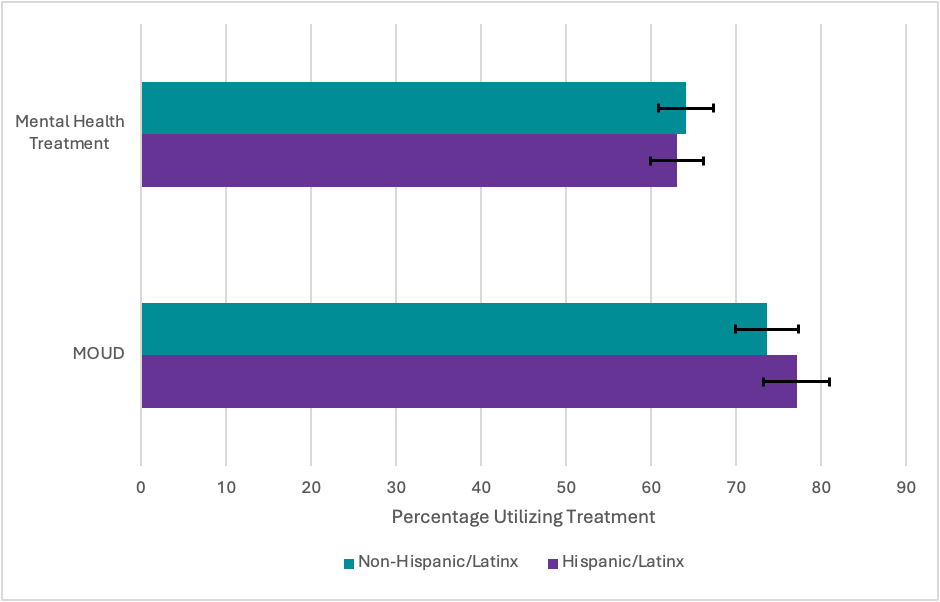
There were no significant differences in mental health treatment or MOUD utilization between Hispanic/Latinx and non-Hispanic/Latinx patients when controlling for age, sex, education, race, marital status, diagnosis group, and health system (Figure 1). Across the full sample, 63.3% of participants reported receiving some form of mental health treatment in the past 30 days, and 76.1% were taking prescribed MOUD as directed in the past 30 days.

4. Discussion
The current study examined differences in utilization of mental health and substance-use treatment between Hispanic/Latinx and non-Hispanic/Latinx patients with OUD and co-occurring depression and/or PTSD receiving primary care. Surprisingly, we identified no significant ethnic differences in utilization of care for OUD, depression, or PTSD in this sample. These results highlight the need for more localized research to identify the drivers of ethnic disparities in health care access and treatment utilization.
Our unexpected findings contrast with the majority of the literature on racial and ethnic disparities in utilization of care for patients with OUD and mental health disorders. Other research has demonstrated that, compared to non-Hispanic white patients, Hispanic/Latinx patients are less likely to receive or be referred to treatment for OUD, and are less likely to have access to MOUD directly in their communities.9–11 Furthermore, Hispanic/Latinx patients are less likely to receive medication for depression, and some evidence suggests that Hispanic/Latinx patients are less likely to receive care for PTSD.24,25
While most of the current literature points to ethnic disparities in access to and utilization of care, some studies have also identified conflicting results. For instance, a 2023 study of reproductive-age women with OUD found that Hispanic/Latinx women are more likely than non-Hispanic white women to begin MOUD treatment, but they are still less likely to complete the treatment.26 Similarly, research suggests that Hispanic/Latinx patients are more likely than non-Hispanic White patients to receive MOUD in long-term care facilities (though less likely in short-term care facilities).27 Such conflicting findings, combined with the findings presented here, demonstrate the need to further investigate contributing factors of ethnic disparities in access to and utilization of care.
Within this discordant research landscape, we must also consider other factors such as geographic location and patient characteristics. New Mexico is one of a few states in which Hispanic/Latinx individuals are a majority group (50.1%), and in 2005, the state began a comprehensive reform of mental health services in an attempt to provide more culturally competent care to fulfill the needs of their population.28 This involved increasing non-English language services and supporting cultural sensitivity training for providers.29 As such, it is conceivable that within New Mexico specifically, utilization of care for Hispanic/Latinx patients is more supported compared to other states. Furthermore, patients included in the CLARO study largely received culturally and linguistically competent care, as most providers in the involved health systems were bilingual and came from the same communities that the health systems served.21 It is therefore possible that, in addition to the statewide landscape, the local clinic-level landscape was especially primed to promote equitable utilization of care. While the effect of these initiatives was not quantitatively examined here, this study highlights the need for dedicated investigation of the impacts of such culturally competent reform, which might lay the groundwork for other states and health care systems to adopt similar programs and practices.
Additionally, it’s possible that certain characteristics of our patient sample may help contextualize our findings. Compared to non-Hispanic/Latinx patients, the Hispanic/Latinx patients in our sample were more likely to report the presence of a significant social support person in their lives. Research suggests that strong social support improves patients’ utilization of and adherence to medical regimens, as involved friends and family provide practical support (i.e., assistance with getting to appointments or picking up medication) as well as emotional encouragement.22 Of course, a broad body of research demonstrates that compared to non-Hispanic White individuals, Hispanic/Latinx individuals are generally more likely to have close and supportive social networks30– but this fact has not mitigated health care disparities observed in other studies.9–11 Thus, more contextualized investigation is required to understand how patient characteristics (including social support) interact with utilization of COD treatment within the specific landscape of individual investigations.
This study contributes a unique perspective to the body of literature by highlighting the experiences of a largely unexplored population – patients with co-occurring OUD plus depression and/or PTSD enrolled in primary care. While our findings contradict much of the literature, this study demonstrates the value of contextualized disparity research, and underscores the importance of further research into the specific and localized manifestations of ethnic health disparities within primary care, so that they can be identified and rectified.
Of course, given that all participants included in the study were receiving primary care at study enrollment, we cannot speak to disparities that may exist in access to primary care itself. However, given that more than 80% of the national population sees a primary care provider at least once a year,31 and that disparities in referral to and utilization of specialty behavioral health services – such as MOUD and mental health treatment – have been documented within primary care, the objective of our study remains pertinent.9–12 Our understanding of ethnic disparities in utilizing mental health and substance-use treatment may be strengthened by future research that includes a comparison between patients established with a primary care provider and patients who do not have a primary care provider.
Beyond this generalizability, a notable limitation of our study involves the way we grouped patients by self-reported race and ethnicity. While the grouping of Hispanic/Latinx has been utilized in a large body of research, it has also been criticized as a white-centric descriptor that obscures important identity-based differences between individuals.32 Country of origin, immigration status, language ability, and other factors all may impact an individual’s experience utilizing health care. Future research must find alternative modes of categorization to consider meaningful subgroup-level differences and identify and rectify any disparities that emerge.
This study contributes to the body of literature concerning ethnic disparities in utilization of health care by highlighting ethnic patterns of utilization for a previously unstudied population: COD primary care patients in New Mexico. While no ethnic disparities were noted in this study, broadly conflicting findings demonstrate the need for more contextualized research in order to rectify any existing discrepancies and improve utilization.
Acknowledgements
This research was supported by a grant from the National Institute of Mental Health/NIMH (U01MH121954). The authors would like to acknowledge the CLARO research team, including our clinic partners at First Choice Community Healthcare, the University of New Mexico Health System, and Hidalgo Medical System. We thank the RAND Survey Research Group staff for their assistance in interviewing and translating materials for patient research participants.
Declaration of Interest
The authors declare that they have no conflict of interest.