Introduction
Type 2 Diabetes (T2D) represents a formidable global health challenge, characterized by its escalating prevalence and profound societal and economic ramifications. In the United States, the burden of this chronic metabolic disorder is particularly pronounced, with its economic costs having surged by 26% between 2012 and 2017, culminating in an estimated $327 billion.1 This substantial figure encompasses both direct medical expenditures and losses related to reduced productivity. Within this broader epidemic, the Hispanic population bears a disproportionately heavy share of the disease. As the largest and most rapidly expanding minority group in the U.S., projected to constitute 29% of the total population by 2050, Hispanic individuals experience significantly elevated rates of diabetes across all age cohorts.1,2 This includes a fivefold higher incidence in children and an 80% higher prevalence in adults compared to non-Hispanic whites (NHWs), highlighting a critical public health disparity that demands urgent attention.1
Nutrition education, which combines educational strategies and environmental supports to promote healthy eating behaviors, is essential for the management and prevention of T2D.3 Diabetes Self-Management Education and Support (DSMES) is recognized as a critical component of care for all individuals with diabetes, and is considered necessary to improve patient outcomes.1 To maximize effectiveness, these programs must be carefully designed to consider the cultural factors that influence the development and progression of diabetes in Hispanic communities.1
However, significant barriers often impede access to and the effectiveness of nutrition education and diabetes management for this population. Low health literacy, defined as the inability to read, comprehend, and interpret health-related information, is a pervasive issue; as many as 62% of Hispanic individuals tested in Spanish have been found to possess low or marginal health literacy.1,2 Compounding this, limited English proficiency acts as a critical barrier to effective patient-provider communication, limiting a patient’s ability to ask questions, verbalize concerns, and establish rapport, which in turn is directly linked to disparities in the quality of care.1 Financial issues also present a formidable obstacle; a substantial 24.4% of Hispanic adults lack health insurance, a rate considerably higher than other racial groups, and 23.9% of Hispanic adults with diabetes reported that the cost of health care was a significant impediment.1
Despite the importance of nutrition education and self-management for diabetic patients, there remains a scarcity of comprehensive data specifically on the nutrition-related knowledge and behaviors of Hispanic subpopulations beyond Mexican Americans.1 This systematic review aims to address this gap by synthesizing current scientific knowledge examining the barriers to nutrition education access among Hispanic adults with T2D. The findings of this review are intended to inform future research, practice, and the development of more culturally tailored interventions for health education programs.
Methods
Research Question
This review was guided by the following research question: “What barriers do Hispanic individuals face when it comes to nutrition education for type 2 diabetes?”
Data Search Strategy
The search strategy used a combination of relevant keywords and Medical Subject Heading (MeSH) terms to identify potential studies. We included peer-reviewed studies written in English that specifically evaluated barriers to nutrition education among Hispanic adults in the United States published between January 2000 and July 2025. We excluded studies in which the population did not focus on adults, was not primarily Hispanic/Latino, or did not include adults with type 2 diabetes.
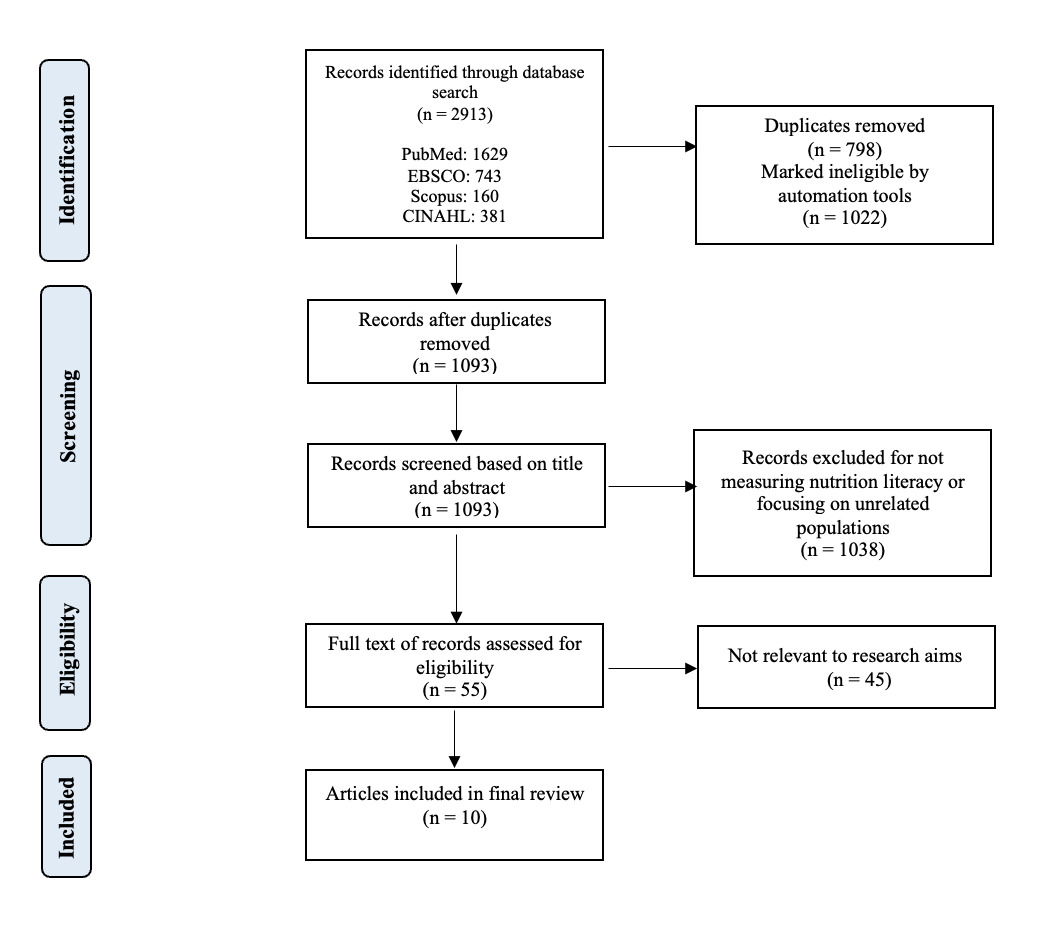
The initial search yielded a total of 2,913 records. These records were imported in Covidence, a systematic review management platform, to facilitate initial screening and collaboration. Covidence highlighted 798 records as duplicates and 1,022 records as ineligible based on title and metadata. A random sample of 50 of those ineligible records was reviewed by two independent reviewers in order to confirm the excluded studies did not meet eligibility criteria. There were no discrepancies between the reviewers. A total of 1,093 articles remained for screening. These articles were then manually screened by title and abstract. During this screening, 1,038 articles were excluded as they did not meet the predefined inclusion criteria.
Therefore, 55 full-text articles were reviewed for eligibility. Ten studies met the inclusion criteria, including 5 qualitative studies, 1 quasi-experimental study, 2 systematic reviews, and 2 mixed-methods studies. The PRISMA flow diagram (Figure 1) summarizes the study selection process.
_diagram__which_.png)
Results
Table 1 summarizes 10 studies of interest for our review. Each study either includes a qualitative or literature review design and evaluates the multiple barriers to nutrition education in Hispanic populations with T2D. This allows us to evaluate the personal experiences, cultural factors, direct interviews, and case studies in different areas of the United States. Commonalities of these studies included a focus on low literacy levels, rural populations, and limited access to health care. All of these factors play a major role in the education and self-care behaviors of those who have T2D.
This systematic review included qualitative, quasi-experimental, literature review, and systematic review studies to support an understanding of barriers faced by Hispanic adults in accessing nutrition education for type 2 diabetes. Given the different methodologies, we used the Mixed Methods Appraisal Tool (MMAT) version 2018 to assess study quality.14 This tool allowed consistent evaluation across various study designs, including qualitative interviews and focus groups, as well as quasi-experimental studies. The MMAT is unable to assess quality of literature and systematic reviews. Studies were evaluated for clarity of research questions, methodological appropriateness, sampling strategy, analytical rigor, and coherence between findings and interpretations. Of the 10 studies, 7 were eligible for MMAT assessment. Overall, 5 studies met all of the MMAT criteria indicating high-methodological quality.
In reviewing the articles, we determined there were key barrier domains to T2D education. Some of these barriers are structural, sociocultural, economic, and psychosocial in nature. Within each of these domains, there are various factors that contribute to the challenges that Hispanic patients with T2D face.
Structural
Structural barriers include systemic issues that populations face in their daily lives, such as poor geographic access to providers, lack of transportation to and from providers, and immigration or documentation issues.7,12,15 Limited resources within an area can greatly impact how well patients can manage their health conditions. Many patients look for free clinics, health care providers that are accessible via public transportation, group programs, and other care options that are low in cost.7,12,15
Sociocultural
These barriers include those that may stem from cultural differences, values, religious practices, language, literacy challenges, or other differences that create disparities among populations. Most prevalent are those challenges of language and literacy barriers within the Hispanic population. To this point, Hu et al states, “one study found that more than half of Hispanic patients with diabetes (52%) had low health literacy, compared to 15% of non-Hispanics with diabetes.”8 These barriers can lead to many issues in managing and finding resources for T2D. Lack of understanding of the language means that people may not be able to read or comprehend medication labels or instructions from their providers. Without the ability to find reliable educational resources, patients may struggle with understanding how to manage their condition properly, leading to possible complications of T2D.
Economic
Economic barriers were reported in most of the studies, highlighting how the cost of healthy foods, food insecurity, and work-related challenges interfere with participation in nutrition education programs. For example, Ramal et al highlighted a direct quote from a study participant about financial constraints that said, “One eats whatever we have at home because there is no money to go and buy what one needs.”9 Other studies also mentioned competing costs such as childcare and transportation as reasons for decreased participation and engagement in diabetes education programs.7,8,11
Psychosocial
Barriers such as emotional distress, stigmas, and attitudes toward managing T2D may also prevent such populations from reaching their health goals and improving management of their condition. Titus et al. highlighted that some patients reported their gender impacted their attitudes toward care.13 For example, one study indicated that “having diabetes suggested to some Hispanic men they lacked machismo (physical strength) and, therefore, delayed getting care.”13 Both this cultural stigma and personal belief can prevent many, especially men, from getting the help they need.
Discussion
This review suggests that Hispanic adults with T2D face complex barriers to nutrition education that extend beyond individual behavior and encompass systemic, cultural, economic, and psychosocial domains.
As we have seen, the barriers to nutrition education for Hispanic populations are vast and extremely prevalent. Of those barriers, language and literacy are among the most challenging issues.
With a different language comes learning, reading, and communication difficulties for those who lack the foundational education they need to obtain information about their disease. Language is the basis for literacy barriers, which may also contribute to difficulties with diabetes management. Without access to education in the primary language of health care delivery, Hispanic individuals face challenges in developing the health literacy skills needed to properly manage diabetes. As such, with a low level of language and literacy comes less knowledge about diabetes and its treatments as a whole. Like Hu et al states, “low literacy was correlated with poorer glycemic control and greater complications related to diabetes. Knowledgeable patients with diabetes are more likely to perform more diabetes self-management activities.”8 These patients are able to read articles, communicate with their provider, and educate themselves on diabetes to understand their disease and what is expected of them for self-care.
Other factors contributing to the language and literacy barriers come within the health care system. Providers who care for patients with diabetes may not be fluent in Spanish, and therefore may not be able to properly educate their Hispanic patients on their own.
Sometimes family members or other staff are needed to help translate, but this is not always possible. And translation alone is not always the most effective solution as medical translation services may not translate health information and facts appropriately.16,17 While translating educational materials does provide information in a patient’s native language, it may not always align with cultural values and beliefs among all Hispanic groups. The tone and content of the material may be impacted by the translation, and the connection between provider and patient may be impacted as there are many different dialects used in the Spanish language. For example, some words in the Spanish language have different meanings in different countries. Because of this, patients may misunderstand the translated information – especially if it is not tailored for their specific cultural context. Research has indicated there is a disconnect between the information delivered by providers and what patients are able to retain or apply in daily life.8,11 This suggests that even when health education is provided in a patient’s native language there are cultural, linguistic, and contextual factors that may impact its effectiveness unless the content is personalized and reinforced through ongoing support.
Structural barriers such as transportation challenges, clinic accessibility, and provider availability also hinder diabetes self-management among Hispanic populations. According to Heuman et al. (2013), many participants in their study identified transportation as a major obstacle to attending medical appointments or diabetes education programs.7 This barrier is especially significant for individuals living in rural or underserved areas, where public transit is limited and distances to clinics are greater. Without reliable transportation, patients are less likely to attend follow-ups or access consistent care, contributing to poor glycemic control and increased risk of complications. Research has shown that telehealth modalities can improve nutrition education engagement for T2D patients.18 Improving patient access to telehealth appointments may help reduce some of these structural barriers.
Structural forces also shape how communities experience their immediate food environment. While the prevalence of ultra-processed foods and sugary beverages in one’s diet may appear to reflect individual choice, those choices are also impacted by media influence and food industry marketing.19 For example, research has shown that television advertisements on Spanish-language channels, including during children’s programming, disproportionately promote low-nutrient, calorie-dense foods and beverages.19 These marketing strategies that propose and promote less-healthy options may make it more difficult to encourage alternatives for improved nutrition without addressing the broader structural determinants.
Clinic accessibility is another critical concern. Clinics often have limited hours that conflict with patients’ work schedules, particularly for those in shift-based or hourly wage jobs.8 Additionally, some patients struggle to find clinics that offer bilingual services, which limits their ability to fully engage with providers and trust in treatment plans. Provider availability also remains inadequate in many underserved Hispanic communities. Participants in multiple studies, including those by Ramal et al. (2012) and Thomas et al. (2017), noted that long wait times, infrequent appointments, and lack of continuity in care undermined their ability to manage diabetes effectively.9,11 These barriers reveal a pressing need for system-level changes, such as extended clinic hours, improved transportation services, greater access to telehealth, and a more diverse and linguistically equipped health care workforce to ensure the best access to diabetes management resources.
Economic constraints were also a near-universal barrier. In addition to cost-related barriers such as lack of insurance or transportation, many of the participants reported food insecurity or feeling like they did not have enough money to buy healthy foods.7,9 Food deserts, or neighborhoods with limited access to affordable nutrient-dense foods, may further restrict patients’ ability to support their health goals.20 Additionally, patients that were working multiple jobs or caring for family members were oftentimes unable to attend nutrition education sessions.8,11 These economic barriers suggest a need for interventions that focus on food access and flexible formats for care such as mobile clinics or after-hours education sessions that don’t interfere with typical work schedules.
Studies have also described emotional or psychological barriers for Hispanic patients with T2D. Patients reported feeling hopeless, lacking motivation, and experiencing shame. These feelings made it harder for patients to want to take part in their care.8,9,11 These barriers may make engagement with nutrition education programs difficult. Interventions that focus on addressing these psychological and emotional barriers, such as motivational interviewing or peer mentoring, may improve participation and outcomes.
It is also important to note that many studies have highlighted how Hispanic women face unique challenges in managing their own health needs as they are often positioned as primary caregivers for the family. Cultural expectations can lead women to prioritize the needs of their children, spouse, or other family members above their own. Unfortunately, doing so may impact their ability to fully engage in diabetes self-management and nutrition education programs.
Researchers have indicated that Hispanic women have limited time, emotional exhaustion, and reduced motivation to focus on self-care activities such as meal planning, exercise, or attending educational sessions.21,22 These findings suggest a need for interventions that recognize the multi-caregiver role many women hold and that offer flexible, family-inclusive formats to better support their participation.
Limitations
This review has several limitations. First of all, some relevant studies may have been missed due to database limitations. Second, the diversity of study designs (qualitative, literature reviews, and experimental) and their differing reporting styles made direct data comparisons difficult. Third, the included studies largely focused on U.S.-based Hispanic populations but varied in terms of national origin (for example, Mexican American, Puerto Rican, Central American), making it difficult to assess how cultural subgroups may experience barriers differently. Additionally, few studies addressed the role of immigration status, trauma, or systemic racism. These factors are also likely to contribute to an individual’s health outcomes. Finally, this review included several qualitative studies, which limits generalizability. The inclusion of more quantitative measures of nutrition education impact would enhance future reviews.
Conclusion
This systematic review highlights the wide range of interconnected barriers that Hispanic adults with T2D face when it comes to accessing and benefiting from nutrition education.
Challenges such as limited transportation, lack of insurance, cultural misunderstandings, financial difficulties, and emotional stress all make it more difficult for individuals to engage in nutrition education programs. To improve the accessibility and effectiveness of these nutrition education programs, future strategies must consider both the content of what is being taught, but also the context in which the education is delivered. Interventions should be culturally tailored with a focus on addressing practical challenges that patients face such as language barriers, time constraints, and financial difficulties.
Expanding both reach and relevance of nutrition education in Hispanic populations will require more than just support at the individual level. Systemic changes in provider training, health care delivery models, and health policies will also be necessary. Additionally, emerging technologies such as social media and artificial intelligence are likely to have a greater influence on the way Hispanic communities access nutrition and diabetes information. Although these technologies may increase access to health information, they also carry the risk of spreading misinformation. Future interventions that utilize digital technologies must consider these factors and confirm the scientific validity of the content before broadly sharing with patient populations. Researchers should focus on developing and evaluating culturally relevant interventions that are tailored to the unique needs of the Hispanic community and the different subgroups within this population.