Introduction
Diversity in medicine has increased the need for representation and inclusion, especially in surgical specialties like Otolaryngology-Head & Neck Surgery (OHNS). The field of OHNS has historically been deficient in representation of racial and gender minorities. This is prevalent in residency programs, in academia, and on a national level in leadership roles. The American Academy of Otolaryngology Head and Neck Surgery (AAO-HNS) Diversity and Inclusion Committee has made it a priority to set initiatives in place to increase racial and gender diversity through mentorship and pipeline programs. Despite small strides, race and gender representation continues to not fully represent the diversity among our own population. This is paramount as women are now the majority in medical schools across the United States.1 Twenty percent of the U.S. population is Hispanic/Latino (HL) and 14% are Black/African American (AA).2 From 2015 to 2024, AA females and HL females showed increased trend of 29.74% and 14.98% respectively in medical school applications.3 This translates to more underrepresented minorities applying to medical schools and postgraduate training programs. However, even though there have been increases in absolute numbers, all racial and ethnic groups remained underrepresented among applicants and matriculants.3 It is important for residency programs to attend to inequities as diversity in the medical workforce has been shown to enhance patient outcomes and cultural competency, reduce language barriers, and increase access to care for underserved communities.4,5 Studies have shown that physicians with minority backgrounds tend to practice in underserved communities, and racial concordance is associated with patient satisfaction, lower mortality rates, and continuation of treatment.6–9
Women surgeons often confront microaggressions and gender-based biases, which affect evaluations and leadership goals.10,11 Underrepresented in Medicine (URiM) report increased discrimination, which can lead to isolation and burnout.12,13 These issues emphasize the need for inclusive OHNS programs to reduce burnout and increase resident well-being. This study examines sociodemographic differences among OHNS residents to shed light on the current landscape and composition of OHNS residency programs.
Methods
This study examines demographic trends across various surgical subspecialty residency programs and in the U.S. Demographic data on residency programs and was obtained from the publicly available Accreditation Council for Graduate Medical Education (ACGME) Data Resource Book for the past five academic years. Data was collected year-by-year starting at 2018-19 up to 2022-23. The targeted population includes all residency program graduates in the U.S. accredited by the ACGME, along with data on applicants to medical school and trends within the physician workforce in surgical subspecialties. Inclusion criteria targeted only data relevant to U.S.-based medical training programs. Primary variables examined include demographic data on residents in surgical subspecialties such as sex, gender, ethnicity, and race. Gender data includes female and male residents. The race/ethnicity examined include non-Hispanic White/Caucasian (WC), Asian, Hispanic/Latino/Spanish (HL), Black/African American (AA), and American Indian/Alaskan Native (AI/AN), with minority populations identified as the latter three groups.14 Demographic data on OHNS residency programs was compared to other surgical subspecialties, including orthopedic surgery, neurosurgery, ophthalmology, and integrated plastic surgery.
To examine the current U.S. population census, data was obtained from the U.S. Census Bureau website.2 To examine trends within the current physician workforce among surgical subspecialties, data was obtained from the Association of American Medical Colleges (AAMC) U.S. Physician Workforce Data Dashboard. To examine data on medical school applicants, data was obtained from the AAMC Medical School Applicants and Matriculant dataset.1
Our primary outcome was change over time in the representation of females and minority residents in OHNS and other surgical subspecialty residency programs from 2018-23. Key measures included year-to-year changes, specialty growth or decline, gender and race growth or decline, and applicant demographics.
Descriptive statistics were utilized to evaluate demographic distribution and sex/gender representation in surgical subspecialty residency programs overtime. Race/ethnicity demographic counts for each academic year from 2018-19 through 2022-23 were tabulated and converted to annual totals and within-year proportions. The “Native Hawaiian” category (all zeros) and the “unknown” categories were excluded from the analysis. An 8-level contingency table of race/ethnicity by year (5 levels) was constructed and a Pearson chi-square test for independence was applied to evaluate whether the distribution of race/ethnicity categories differed across years. For sex/gender, yearly counts were similarly totaled and expressed as proportions. Variables such as “nonbinary” and “not reported” contained few observations and were grouped into another category, yielding a three-level analysis. A Pearson test of independence was then conducted using the same significance threshold. Statistical significance was assessed at a two-sided α of 0.05. All analyses were performed using GraphPad Prism version 10.3.1.15
A systematic PubMed search was conducted to include data regarding residency program structures, training outcomes, and case assignments amongst demographics in OHNS. National residency survey questionnaires and cohort study data from previous studies were analyzed to highlight factors contributing to bias and discrimination toward those underrepresented in OHNS.16,17
Results
Residency Program Data
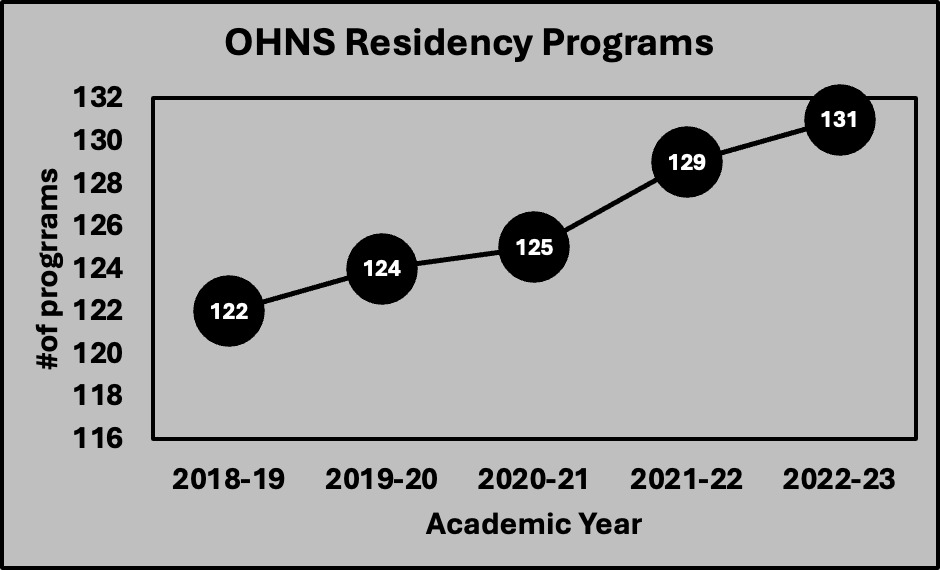
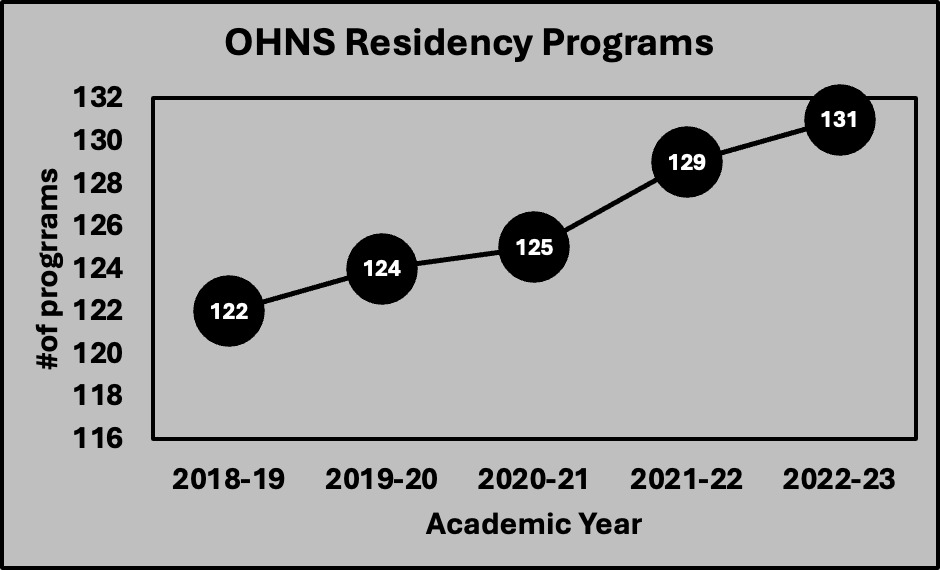
The number of OHNS residency programs increased by 7.4% from 2018 to 2023, expanding from 122 to 131 [Figure 1]. This translates to an increase from 1,651 OHNS residency positions to 1,795. Of the 1,795 ENT residents in 2022-23, 764 were female.
Race/Ethnicity Data
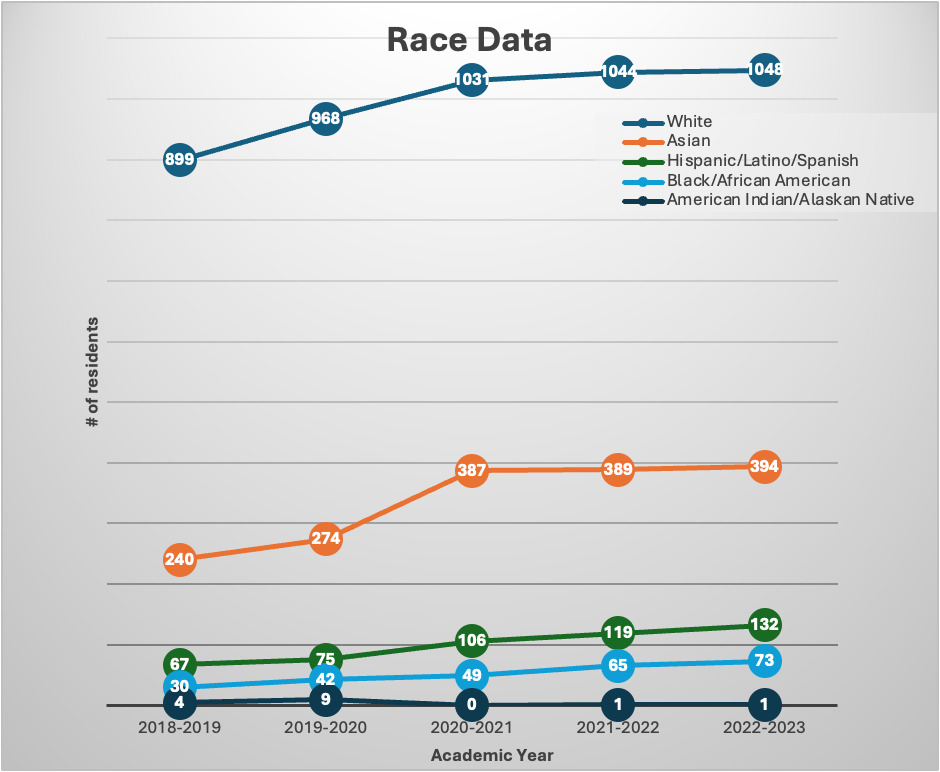
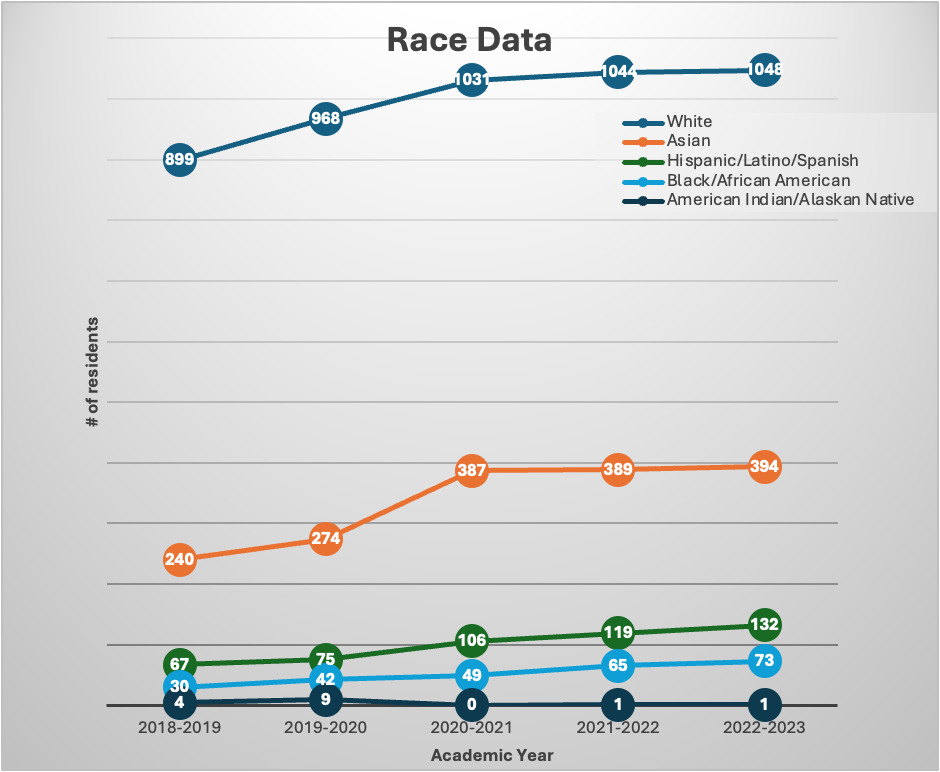
AA student representation increased by 8.1% and HL student representation increased by 6.4%. The percentage of AA OHNS residents increased to 4.1% in 2022-23 from 1.8% in 2018-19. The percentage of HL ENT residents increased to 7.4% in 2022-23 from 4.1% in 2018-19. Between 2018 and 2023, there has been a 143% increase in AA residents and a 97% increase in HL residents. AI/AN residents represented less than 1% of all OHNS residents. [Figure 2] The Pearson chi-square test of independence comparing racial distributions across five academic years resulted in = 119.1, df = 24, p<0.001, which indicates that the overall race/ethnicity composition of the trainee cohort changed significantly over time. WC trainees remained the majority of the demographic groups and showed an increase of 16.6% between 2018 and 2023.
Sex/Gender Data
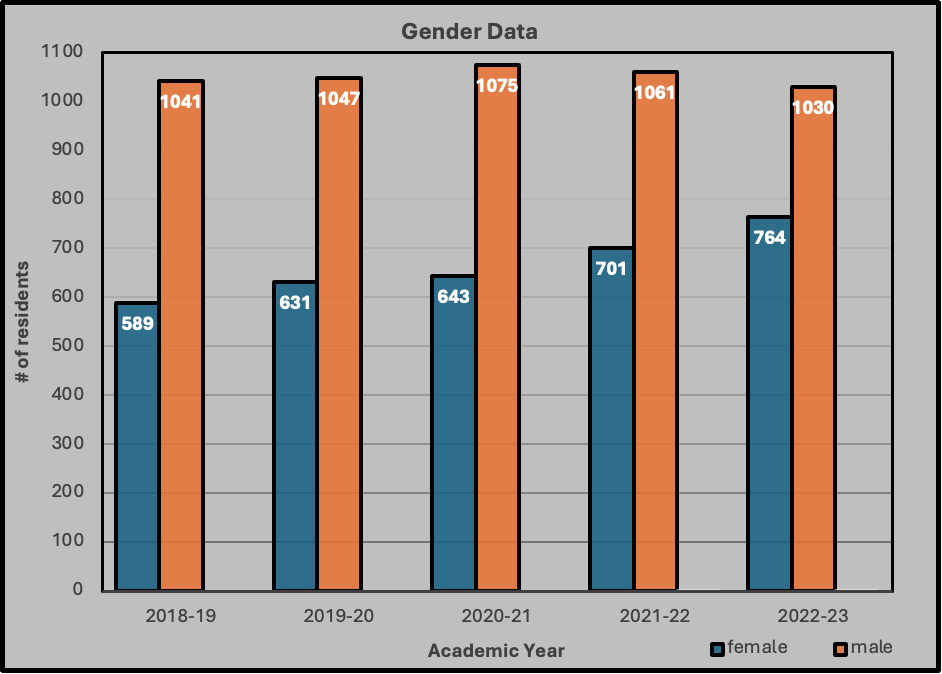
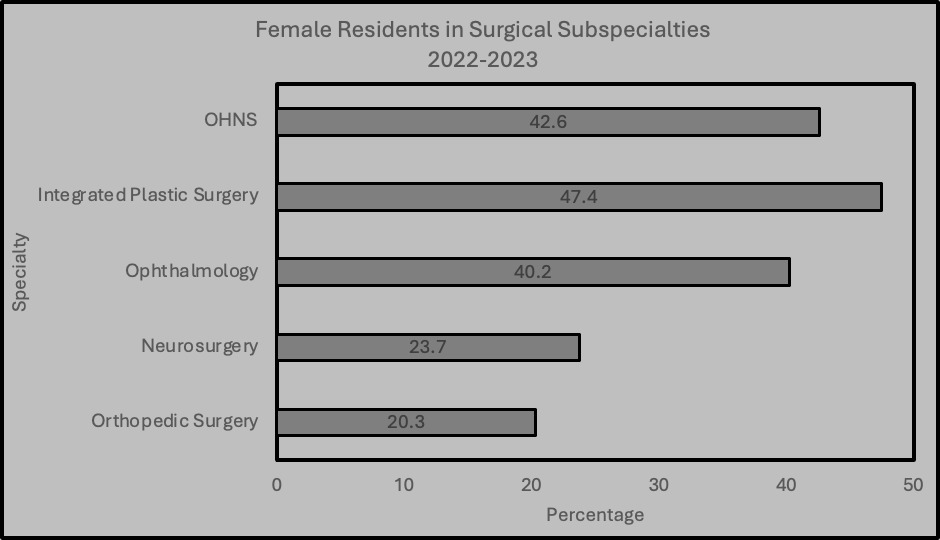
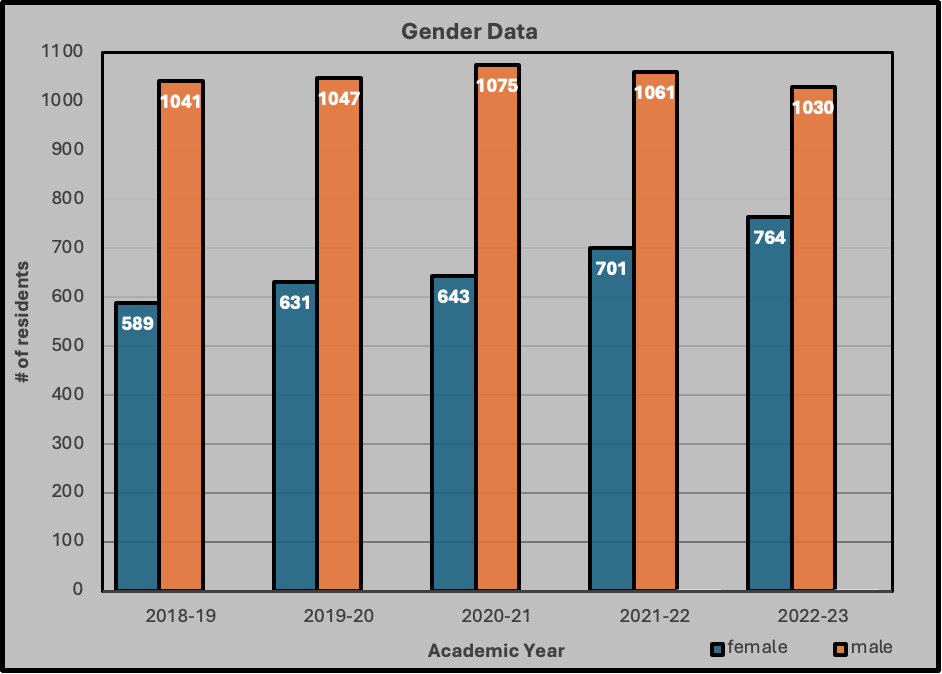
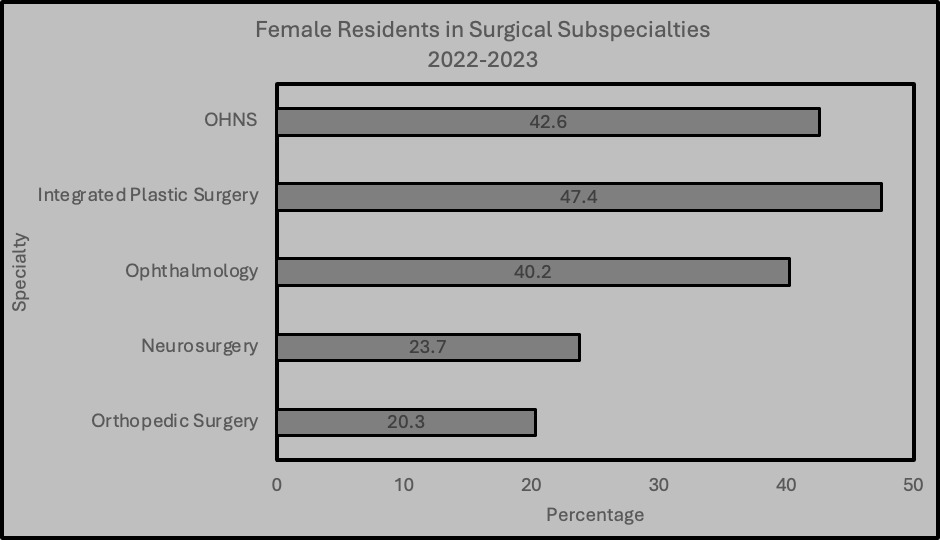
The proportion of female OHNS residents has persistently increased over the last five years. In 2023, women made up 53% of all U.S. medical students. The percentage of female OHNS residents increased from 36.1% in 2018-19 to 42.6% in 2022-23. This reflects a 30% increase in the number of female OHNS residents since 2018. [Figure 3]. In 2022-23, the percentage of female OHNS residents (42.6%) was lower than the percentage of integrated plastic surgery female residents (47.4%), but higher than ophthalmology (40.2%), neurosurgery (23.7%), and orthopedic surgery (20.3%) [Figure 4]. The Pearson chi-square test of independence comparing race/ethnicity distributions across five academic years resulted in = 92.37, df = 4, p<0.001. This shows that the overall sex/gender composition of the trainee cohort also changed significantly over time.
HL and AA residents in surgical subspecialties
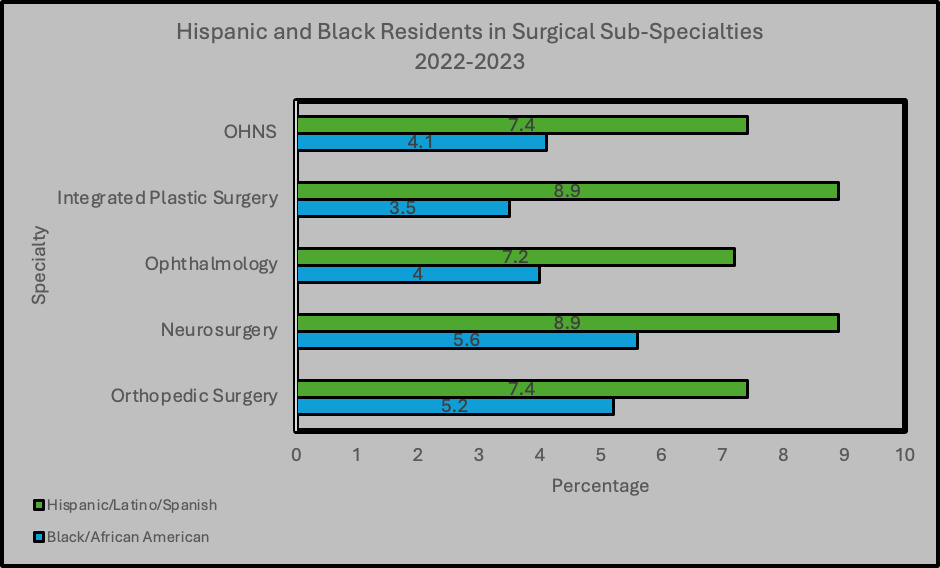
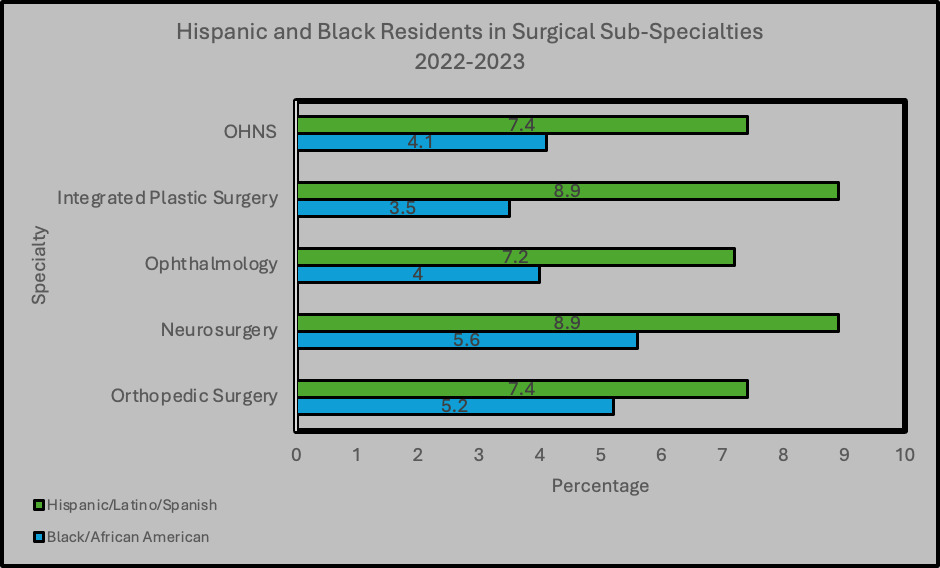
The percentage of AA OHNS residents (4.1%) was less than neurosurgery (5.6%) and orthopedic surgery (5.2%), but higher than ophthalmology (4.0%), and integrated plastic surgery (3.5%). The percentage of HL OHNS residents (7.4%) was less than integrated plastic surgery (8.9%) and neurosurgery (8.9%), similar to orthopedic surgery (7.4%), and greater than ophthalmology (7.2%) [Figure 5].
Discussion
Diversity in medicine has increased the need for representation and inclusion, especially in surgical specialties like OHNS. The AAO-HNS has made progress, yet gaps remain. Racial and gender inequalities affect resident experiences, recruitment, retention, and even performance. These inequalities can undermine resident physicians’ well-being and the quality of care for different patients.4,11,12
Between 2018 and 2023, there was a noticeable shift in OHNS residency programs. These changes were observed both in the quantity of programs as well as resident diversity. The number of programs increased by 7.38%, expanding from 122 programs to a total of 131 by the end of this period. This change also brought a rise in representation for historically marginalized populations. Of these, AA residents surged by 143%, while HL resident representation increased by 97%. Looking further into this, we found that this trend was also apparent as we looked at the representation of these populations in the medical student cohorts. AA student representation increased by 8.1% and HL student representation increased by 6.4%. Sex and gender diversity also saw an increase with a record high of 42.6% female resident representation in 2023, a 30% increase since 2018.
When we compare this to other surgical fields, we see that OHNS has achieved a higher degree of diversity than fields like ophthalmology and integrated surgery. OHNS has seen a greater proportion of AA residents in 2023, increasing from 1.8% in 2018 to 4.1%. Nevertheless, it is still trailing behind neurosurgery and integrated plastic surgery for HL representation. The rise in sex/gender diversity among OHNS residencies aligns with the trends seen nationwide.
The difference in female representation in OHNS (42.6%) stands out in comparison with other competitive fields such as orthopedic surgery (20.3%) and neurosurgery (23.6%). Ophthalmology came close to OHNS with 40.1% of residents being female. This suggests focused initiatives aimed at enhancing gender diversity might be producing positive outcomes across multiple fields. In 2023, women made up 53% of all U.S. medical students. This change mirrors the health care sector’s emphasis on gender equality and has had a beneficial influence on the makeup of residency programs.
These changes in cohort composition may be a result of the efforts made by the AAO-HNS Diversity Committee, which, since 2007-08, has invested time and money into tools that have been proven to increase equity in other areas of medicine.18 For example, the W. Harry Barnes Endowment and the Diversity Endowment have created opportunities and allocated funds for minority students to travel to audition rotations, conferences, and residency interviews through travel grants. Additionally, they have created diversity committees with individuals who are passionate about this subject and are actively working to implement strategies to diversify the field.19 The AAO-HNS also sponsors similar activities by providing their own travel grant for URiM.20 Nevertheless, apart from these specific specialty-led initiatives, the observed increase trends are most likely multifaceted, influenced by the global events of 2020.
Mentorship, interviews, and ranking all have strong effects on determining OHNS candidates for residency and further diversity in the field. Supporting URiM students through these efforts and milestones have been proven to not only have a real impact on residency cohorts but also provide a sense of unique support that can only be achieved through representation in medicine. Mentorship provides tangible and intangible support, connecting trainees to research, projects, funding, and professional networks. Mentors can validate the trainee’s identity and aspirations, offer encouragement in moments of doubt, and model what a successful career can look like for someone of a similar background. The role of professional sponsorship and personal affirmation has been described as a crucial factor in why mentorship disproportionately benefits women and URiM trainees. In this sense, mentorship is a structural intervention to promote equity within OHNS.4,21,22
Although these developments show forward progress, it is important to acknowledge certain constraints. Primarily, the information at hand does not seek to understand the root reasons behind the changes noticed, like recruitment strategies, shifts in application trends, or organizational regulations focused on promoting inclusion. Moreover, while there has been a rise in the number of minority residents, their proportional representation is still underrepresented when compared to the general population.4,5,7 There might also be differences among residency programs that are not reflected in the overall data analysis, as this analysis was obtained through publicly available data that may not always be entirely accurate due to limitations in self-reporting.
It is important not only to pave a path forward to address the disparities in representation among resident physician cohorts, but also to address the challenges that they face in residency. Burnout prevalence among resident physicians is 50%, with OHNS residents experiencing burnout at a rate of 58.6%.23 Long work hours with minimal institutional support can cause emotional weariness, and racial and gender bias exacerbate it. Women surgeons often confront microaggressions and gender-based biases, which affect their evaluations and leadership goals. URiM report increased discrimination, which can lead to isolation and burnout. More importantly, having more women in the field created opportunities for mentorship, which has proven to be a strong contributor to students entering the medical field and matching into residency.24 Mentorship and reverse mentoring can help marginalized residents thrive personally and professionally. Outreach to high-level medical and college students may also help further diversify the sector by finding and developing talent. Diversifying OHNS is ethical and enhances patient care as URiM physicians are more likely to serve underserved populations and build trust among these communities.4
Limitations
Our analysis is limited by the sample size and the use of two points for comparison. Even though this approach allows for preliminary inferential analysis, it does not capture the complete trajectory of change and trends in sex/gender or race/ethnicity representation over time within OHNS residency programs. Additionally, the dataset did not contain cross-tabulated demographic information, which prevented intersectional group analysis. Nevertheless, this study provides a foundation for future research through meaningful insight into the state of diversity and highlights areas that warrant continued monitoring not only in the OHNS field, but also in other surgical subspecialties. Future studies should incorporate multiple time points across longer intervals and additional medical training careers like general surgery to allow a more detailed assessment while building on the observations reported here and exploring intersectional patterns.
Conclusion
This study demonstrates that the OHNS field has comparatively greater trends of increased representation of URiM relative to other surgical subspecialties. The positive developments in promoting diversity and gender balance are promising. Maintaining this improvement requires ongoing dedication. Studies on the underlying reasons for OHNS program representation disparities are needed. Program-level diversity initiatives should also be studied. Lawmakers, educators, and residency program administrators should prioritize ways to attract and support underrepresented groups, whether that includes racial, gender, socioeconomic status considerations, or all the above.